Understanding leads ecg placement is crucial for accurate heart diagnostics. Whether you’re a medical student, nurse, or physician, mastering this skill ensures reliable ECG readings and better patient outcomes. Let’s dive into the essentials.
What Is Leads ECG Placement and Why It Matters

Leads ecg placement refers to the precise positioning of electrodes on the body to record the heart’s electrical activity. An electrocardiogram (ECG or EKG) uses 12 different leads—each offering a unique view of the heart’s function. Incorrect placement can lead to misdiagnosis, including false positives for myocardial infarction or arrhythmias.
The Science Behind ECG Leads
The heart generates electrical impulses that travel through cardiac tissue, causing contractions. These signals are detected by electrodes placed on the skin. The standard 12-lead ECG combines three types of leads: limb leads, augmented limb leads, and precordial (chest) leads. Each provides a different angle of the heart’s electrical vector.
- Limb leads (I, II, III) measure electrical activity in the frontal plane.
- Augmented limb leads (aVR, aVL, aVF) enhance signal strength from unipolar recordings.
- Precordial leads (V1–V6) capture horizontal plane activity across the chest.
“Accurate leads ecg placement is the foundation of reliable cardiac diagnosis.” — American Heart Association
Common Errors in Leads ECG Placement
Misplaced electrodes are among the most frequent errors in clinical practice. Studies show up to 40% of ECGs have at least one lead misplaced. Common mistakes include:
- Placing V1 and V2 too high or too low on the sternum.
- Rotating the precordial leads due to incorrect intercostal space identification.
- Swapping left and right arm electrodes, which reverses lead I and alters the entire axis interpretation.
These errors can mimic conditions like ischemia, hypertrophy, or bundle branch blocks. For example, misplaced V1 can create a false appearance of right bundle branch block (RBBB), leading to unnecessary testing.
Step-by-Step Guide to Correct Leads ECG Placement
Proper technique is essential for diagnostic accuracy. Follow this standardized method for leads ecg placement to ensure consistency and reliability.
Positioning the Limb Electrodes
The four limb electrodes form the basis of the hexaxial reference system. They should be placed on the right and left wrists and ankles—or on the upper arms and lower legs if limb amputations exist.
- RA (Right Arm): Place on the right forearm, near the wrist.
- LA (Left Arm): Place symmetrically on the left forearm.
- RL (Right Leg): Acts as the electrical ground; place on the right lower leg.
- LL (Left Leg): Place on the left lower leg, opposite the right.
Ensure the skin is clean and dry. Avoid bony prominences and large muscles to reduce artifact. According to the American Heart Association, consistent placement improves waveform reproducibility.
Locating the Precordial Leads (V1–V6)
The chest leads are the most vulnerable to misplacement. Here’s how to locate them accurately:
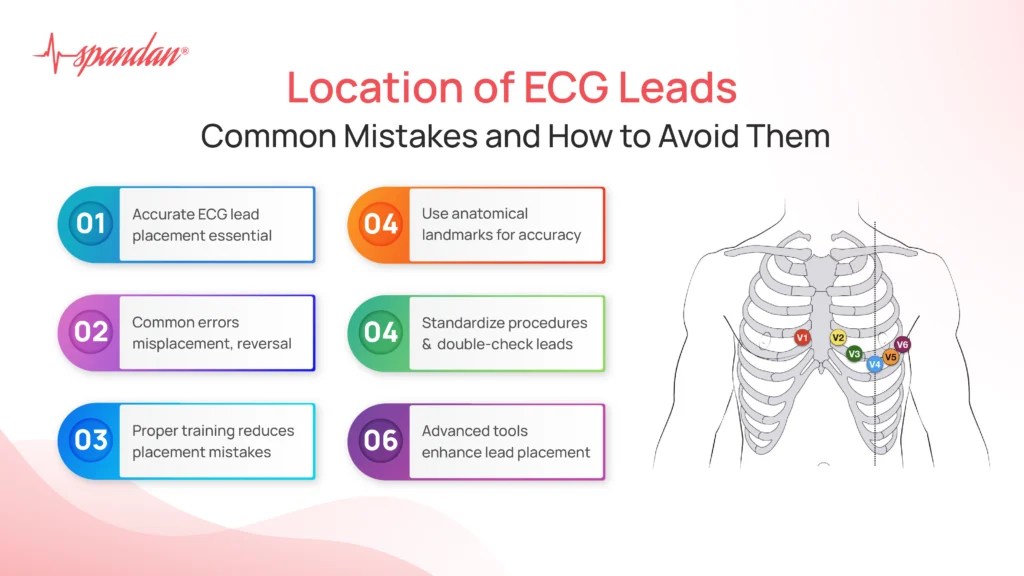
- V1: 4th intercostal space, right sternal border.
- V2: 4th intercostal space, left sternal border.
- V3: Midway between V2 and V4.
- V4: 5th intercostal space, midclavicular line.
- V5: Same horizontal level as V4, anterior axillary line.
- V6: Same level as V4, midaxillary line.
Use anatomical landmarks: the angle of Louis (sternal angle) marks the 2nd rib. From there, count down to the 4th intercostal space. Misidentifying this space is a common error, especially in obese or edematous patients.
Special Considerations for Women and Obese Patients
In women with large breasts, V3–V6 should be placed on the chest wall beneath the breast, not on the breast tissue itself. Suspend the breast if necessary to access the correct anatomical position. For obese patients, use extra lead adhesive or gel to ensure contact. Some clinicians use a breast displacement technique validated by research in the National Institutes of Health.
The Impact of Incorrect Leads ECG Placement on Diagnosis
Misplaced leads can distort the ECG waveform, leading to clinical misinterpretation. Even small deviations—just one intercostal space—can alter the appearance of the QRS complex, ST segment, and T wave.
How Misplacement Mimics Myocardial Infarction
Incorrect placement of V1 and V2 can create QS waves in the right precordial leads, mimicking anterior myocardial infarction. A study published in Journal of Electrocardiology found that 30% of ECGs with misplaced V1 showed abnormal Q waves indistinguishable from true infarction patterns.
- High placement of V1/V2 increases R-wave amplitude in V1, suggesting posterior MI.
- Low placement flattens R-wave progression, mimicking anterior ischemia.
- Lateral lead misplacement (V5/V6 too high) can simulate inferior ST elevation.
“A misplaced ECG lead can send a patient to the cath lab unnecessarily.” — Dr. William A. Zoghbi, American College of Cardiology
Axis Deviation Due to Limb Lead Reversal
Reversing right and left arm electrodes causes lead I to invert, making the QRS complex negative. This mimics extreme axis deviation or dextrocardia. Lead II and III also swap, altering the appearance of P waves and QRS morphology.
- Right arm/left arm reversal: Inverted P and QRS in lead I.
- Right arm/left leg reversal: Can mimic inferior MI.
- Left arm/left leg reversal: Minimal change but may affect axis calculation.
Always check for these patterns. If lead aVR shows a positive QRS (which is normally negative), suspect limb lead reversal.
Advanced Techniques in Leads ECG Placement
Beyond the standard 12-lead setup, advanced techniques improve diagnostic yield in specific conditions. These include posterior leads, right-sided leads, and high intercostal placements.
Posterior Leads (V7–V9) for Posterior MI Detection
Posterior myocardial infarction often goes undetected on standard ECGs. Adding posterior leads increases sensitivity:
- V7: 5th intercostal space, posterior axillary line.
- V8: Same level, mid-scapular line.
- V9: Same level, paraspinal area.
These leads detect ST elevation in posterior MI, which appears as ST depression in V1–V3. According to American College of Cardiology guidelines, posterior leads should be considered in patients with suspected inferior or lateral MI.
Right-Sided Leads (V3R–V6R) for Right Ventricular Involvement
In right coronary artery occlusion, right ventricular infarction may occur. Right-sided leads help detect this:
- V3R: Mirror position of V3 on the right side.
- V4R: 5th intercostal space, right midclavicular line (most important).
- V5R/V6R: Continue to right anterior and midaxillary lines.
ST elevation in V4R is a strong predictor of right ventricular infarction and guides fluid management. This technique is recommended in Braunwald’s Heart Disease as a critical adjunct in acute MI evaluation.
High Intercoastal Placement for Atrial Abnormalities
In cases of suspected atrial enlargement or ectopic atrial rhythms, placing V1 higher (2nd or 3rd intercostal space) can better capture P-wave morphology. This is particularly useful in diagnosing ectopic atrial tachycardia or P-pulmonale.
Training and Education in Leads ECG Placement
Despite its importance, leads ecg placement is often taught inadequately. Medical students and new nurses frequently receive minimal hands-on training, leading to persistent errors in clinical practice.
Simulation-Based Learning
High-fidelity simulators and mannequins allow learners to practice electrode placement repeatedly. Institutions like Johns Hopkins use ECG simulation labs where students receive real-time feedback on lead positioning accuracy.
- Visual feedback systems highlight incorrect placements.
- Auditory cues confirm correct intercostal space identification.
- Software compares student-placed leads with gold-standard positions.
A study in Medical Education Online showed a 60% improvement in placement accuracy after simulation training.
Certification and Competency Assessment
Hospitals should implement mandatory competency checks for ECG technicians. The American Heart Association recommends annual re-certification for all staff performing ECGs. This includes:
- Written exam on lead anatomy and placement.
- Practical test on a live model or simulator.
- ECG interpretation quiz focusing on artifact recognition.
Such programs reduce diagnostic errors and improve patient safety.
Technology and Innovation in Leads ECG Placement
Emerging technologies are transforming how we approach leads ecg placement, reducing human error and improving consistency.
ECG Wearables and Smart Patches
Devices like the Zio Patch and Apple Watch ECG offer single-lead recordings, but new multi-lead wearable systems are in development. These use adhesive arrays with pre-positioned electrodes, minimizing placement variability.
- Pre-gelled, fixed-distance electrodes ensure correct spacing.
- Bluetooth-enabled patches transmit data directly to EMR.
- AI algorithms flag potential misplacements before analysis.
The FDA has approved several such devices, including the Forest Medical 12-lead wearable, which uses a vest with embedded sensors.
Augmented Reality (AR) for Training
AR applications overlay virtual electrodes onto a patient’s body via tablet or smart glasses. Trainees see exactly where to place each lead, guided by anatomical landmarks. This technology is being piloted at Mayo Clinic and has shown a 75% reduction in initial placement errors.
AI-Powered Placement Verification
Machine learning models can now analyze ECG tracings to detect lead misplacement. For example, an algorithm developed at Stanford can identify right arm/left arm reversal with 98% accuracy by analyzing P-wave direction in lead I and aVR.
- Real-time alerts during ECG acquisition.
- Integration with hospital ECG machines.
- Automated report flagging: “Possible V1/V2 misplacement.”.
This innovation promises to make leads ecg placement more reliable across settings.
Global Standards and Guidelines for Leads ECG Placement
While the basic principles are universal, slight variations exist between countries. Harmonizing standards improves data comparability and patient care.
AHA, ESC, and ACC Recommendations
The American Heart Association (AHA), European Society of Cardiology (ESC), and American College of Cardiology (ACC) jointly published standardized guidelines in 2009, reaffirmed in 2020. Key points include:
- Electrodes should be placed on the torso for limb leads in obese patients.
- Use of conductive gel or pre-gelled electrodes to reduce impedance.
- Documentation of any non-standard placement (e.g., “limb leads on shoulders”).
These guidelines are available at ESC’s official website.
ISO Standards for ECG Equipment
The International Organization for Standardization (ISO) sets technical requirements for ECG machines and electrode design. ISO 1351:2014 specifies electrode color coding:
- RA: White
- LA: Black
- RL: Green (ground)
- LL: Red
- Chest: Brown (V1–V6)
Adherence to these standards prevents confusion and enhances safety.
Cultural and Regional Variations
In some countries, limb leads are placed on the shoulders and hips instead of arms and legs. While acceptable, this alters waveform amplitude and must be noted. Japan traditionally uses a different chest lead configuration, though most now follow international standards.
Best Practices for Ensuring Accurate Leads ECG Placement
To minimize errors and maximize diagnostic value, follow these evidence-based best practices for leads ecg placement.
Pre-Procedure Checklist
Before attaching electrodes, perform a quick checklist:
- Verify patient identity and indication for ECG.
- Expose the chest fully; remove excessive hair if needed.
- Clean skin with alcohol wipes to reduce impedance.
- Palpate the angle of Louis to locate the 2nd rib.
- Mark V4 first (5th ICS, midclavicular line), then work backward.
This systematic approach prevents rushing and ensures accuracy.
Double-Check and Peer Review
After placement, visually inspect all electrodes. Ask a colleague to verify if possible. Many hospitals use a “two-clinician check” for critical ECGs, especially in emergency settings.
Documentation and Communication
Always document any deviations from standard placement. For example: “LL lead placed on left thigh due to leg edema.” This helps interpreters adjust their analysis accordingly.
- Include patient position (supine, semi-Fowler’s).
- Note time of day and recent activity.
- Flag technical issues on the ECG printout.
Clear documentation supports continuity of care and medico-legal safety.
What is the correct placement for V1 in leads ecg placement?
V1 should be placed in the 4th intercostal space at the right sternal border. This is a critical landmark, as incorrect placement here can mimic right ventricular hypertrophy or anterior myocardial infarction.
What happens if limb leads are reversed during leads ecg placement?
Reversing right and left arm leads causes lead I to invert, making the QRS complex negative. This can mimic dextrocardia or extreme axis deviation. Always check for a positive QRS in aVR, which suggests this error.
How can technology improve leads ecg placement accuracy?
Technologies like augmented reality (AR), AI-powered verification, and pre-configured wearable patches help reduce human error. These tools provide real-time feedback and standardize electrode positioning across different operators.
Why is leads ecg placement important for diagnosing heart attacks?
Accurate leads ecg placement ensures that ST-segment changes, Q waves, and T-wave inversions are correctly identified. Misplacement can mimic or mask myocardial infarction, leading to delayed treatment or unnecessary interventions.
Are there special leads ecg placement techniques for women?
Yes. In women with large breasts, precordial leads V3–V6 must be placed on the chest wall beneath the breast, not on the breast tissue. This prevents signal attenuation and ensures accurate R-wave progression.
Mastering leads ecg placement is a fundamental skill that directly impacts patient care. From proper limb and chest electrode positioning to understanding the consequences of errors, every detail matters. With advances in training, technology, and global standards, we can reduce variability and improve diagnostic accuracy. Always follow best practices, double-check your work, and stay updated with guidelines to ensure life-saving precision in every ECG you perform.
Recommended for you 👇
Further Reading: